

On May 2, 2022, Politico released a leaked draft of the Supreme Court’s majority opinion[1] in the case of Dobbs v. Jackson Women’s Health Organizations overturning Roe v. Wade. Penned by Justice Samuel Alito in February 2022, the draft argued that abortion is not a constitutional right, as previously established by 1973’s Roe decision. Instead, the draft held that individual states have the power to legislate a person’s right to an abortion. In June 2022, a majority of Supreme Court justices signed onto Justice Alito’s draft majority opinion, sending the legal status of abortion back to each state. In the following days and weeks, thirteen U.S. states with trigger laws enacted debilitating requirements or all-out bans on abortion access. Due to the decisions of five unelected justices, decades of previous federal protection to terminate an unwanted, dangerous, or forced pregnancy was eliminated.
In response to the ruling, reproductive rights activists mobilized immediately. Protests erupted in every major U.S. city, as well as in cities around the world, fueled by people who abhorred the Supreme Court’s swift decision to set women’s rights back a half century. The impassioned response was no surprise, but the protestors (while numerous) hardly represented all of those who were upset by Roe’s overturning. The Pew Research Center reports that 61% of U.S. adults believe that abortion should be legal “all or most of the time,”[2] meaning that abortion is broadly supported by U.S. citizens.
Abortion Demographics
Abortion is a common procedure. According to the Guttamacher Institute, which researches and advocates for sexual health and reproductive rights, about 3 in 10 women in the U.S. will have an abortion by age 45. People of different genders, ages, races, ethnicities and religions receive abortions. According to Guttmacher, 60% of these patients are in their 20s (only 12% are teens); 59% of already have children; 39% identify as white, 28% identify as Black, 25% identify as Hispanic, 6% identify as AAPI, and 3% identify as a different race; and 62% of these patients self-identify as religiously-affiliated.[1]
In general, abortions performed by qualified health care professionals are safe procedures. According to Guttmacher, fewer than 1 in 200 women will experience a complication from an abortion, which is far less than the rate of complications experienced in childbirth.
Many people do not know that, for the first 10 weeks of pregnancy, people can terminate a pregnancy by taking prescribed medication alone. The medications, Mifeprex and Mifepristone, work together to cause cramping (similar to menstrual cramps) which expel an embryo from the uterus. The entire process takes 24-72 hours and is between 93-98% effective at terminating pregnancy, depending on the gestational age. Abortions later in pregnancy (more than 10 weeks gestation) are considered “surgical,” where a providers use suction or dilation/evacuation techniques to complete an abortion.[1]
Although people of all different backgrounds have abortions, 75% of abortion patients are considered poor or low-income. This means that people with fewer financial resources tend to receive proportionately more abortions than people with greater financial resources. Compounding this higher risk of needing an abortion are increased barriers to obtaining/paying for abortions for lower-income folks. The Hyde Amendment, passed in 1976, denies abortion coverage to people receiving Medicaid or Medicare, federal employees and their children, Peace Corp volunteers, indigenous people who receive care through the Indian Health Services, people in federal prisons, military members/veterans or their children, or low-income folks living in D.C.[2]
In other words, the Hyde Amendment allows anti-choice legislators to deny people who rely on federal funds for their health care – a large percentage of the population – from using their health insurance to obtain an abortion. Because abortions are generally expensive procedures, anywhere from a few hundred to a few thousand dollars, the Hyde Amendment severely limits lower-income patients from receiving abortions.
Abortion in North Carolina
The power to legislate the right to an abortion is now in the states’ hands, which means that access to abortion is incredibly varied from state to state. There are many ways in which a state can choose to protect or restrict a person’s access to abortion, even without banning abortion entirely.
Guttamacher identifies that following categories of restrictions:[1]
- Refusal: 45 states allow individual health care providers to refuse to participate in an abortion.
- Parental Involvement: 36 states require parental involvement in a minor’s decision to have an abortion.
- Waiting Periods: 24 states require a patient to wait a prespecified period of time after receiving counseling on abortion to then receive an abortion.
- Public Funding: 33 states prohibit the use of state funds to pay for abortions for Medicaid enrollees unless the patient’s life is in danger or the pregnancy is a result of rape/incest.
- Gestational Limits: 43 states prohibit abortions after a specific point in pregnancy.
States use restrictions in different ways to discourage or prevent people who are pregnant from receiving abortions. Guttmacher published the map below to visualize these differences:
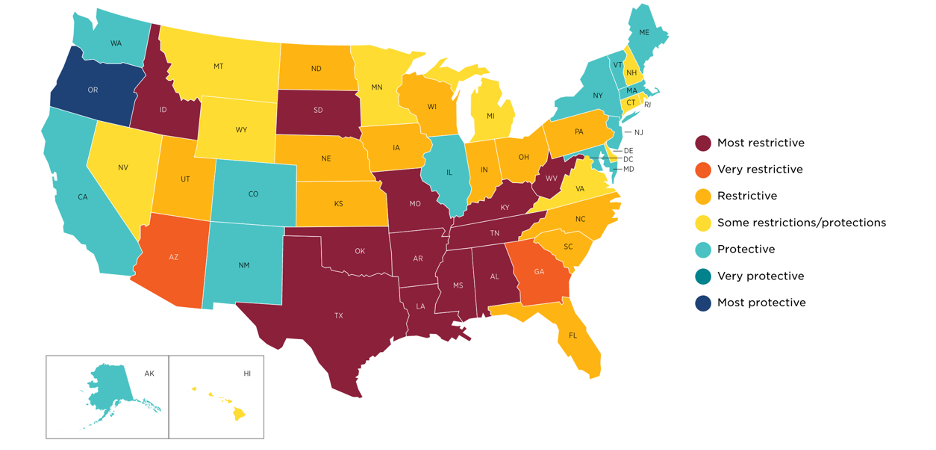
North Carolina is categorized as generally “restrictive” towards abortions. In the state, people who are pregnant are subject to the following restrictions when seeking an abortion:
- Abortion is banned after 20 weeks and 6 days gestation.
- Patients must wait 72 hours after counseling to receive an abortion.
- State Medicaid coverage of abortion is banned (of note, 15% of North Carolinian women aged 15-49, a total of 360,000 people, are insured by Medicaid).
- Medication for abortion must be provided in-person because the use of telehealth/mailed medication in abortion counseling alone is banned.
- Parental consent is required for a minor’s abortion.
- Only physicians can provide abortions, not other qualified health care professionals.[1]
[1] https://states.guttmacher.org/policies/north-carolina/abortion-policies
Resources for Pregnancy-Capable People in North Carolina
- If you are considering an abortion:
- If you need help finding an abortion provider:
- If you need help paying for an abortion:
Given the U.S.’s hostile environment towards abortion, it is more important than ever to protect yourself against unwanted pregnancy. Consider long-acting reversible contraception (LARCs) such as implants or IUDs, which are hands-down the most effective at preventing unwanted pregnancy. These can be ordered and placed at most OB/GYN clinics and some pediatric clinics.
- Information on IUDs.
- Information on implants.
Reminder to EVERYONE!
Remember to VOTE in the North Carolina midterm elections, which are fast approaching on Tuesday, November 8th. Although ballots will vary from county to county, all registered North Carolina citizens will have the chance to vote for a new senator to represent our state in the U.S. Senate. The two main candidates running are Democrat Cheri Beasley and Republican Ted Budd. For your information: Beasley supports additional protections to abortion access; Budd supports additional restrictions on abortion access.
- Read about each candidate on your ballot:
- Request an absentee ballot:
- Find out where to vote on November 8th:
There are no comments
Add yours